

What is a Spinal Cord Injury?
The spinal cord is a bundle of nerve cells (neurons), their fibers (axons), and supporting cells (glial cells), which begins at the bottom of the brain stem and ends in the lower back (at the first-second lumbar vertebra of the spinal column). The spinal cord lies inside the spinal column and is protected by the vertebrae. This bundle of nerve cells and fibers connects the brain and the rest of the body by mediating nerve signals (sensory, motor, and autonomic) from the brain to the body organs and back. Such signals enable us to move our limbs, detect sensations like pain, heat, cold, and touch, perceive the positioning of our body in space and mediate autonomic (involuntary) functions of the body, such as digestion, breathing, heart function, bladder function, muscle contraction, and relaxation, etc.’
A spinal cord injury (SCI) is one of the most common causes of disability in the world, involving damage to the bundle of cells and nerve fibers, which means that some or all of the nerve signals may not be able to get through from the brain to the rest of the body. The result is a complete or partial loss of sensation, mobility, and autonomic function below the level of the injury. In most cases, a SCI involves a severe physical trauma that is likely to significantly and continuously impact many physical and functional aspects of daily life. The most common causes of SCIs are road accidents, falls, acts of violence, sports injuries, and domestic accidents.
The Extent of Disability
The extent of disability will depend on the location of the injury along the spinal cord as well as its severity. As mentioned, the spinal cord consists of millions of nerve cells which are divided into 31 pairs of spinal nerves, grouped regionally by spinal segments: 8 cervical nerve pairs, 12 thoracic nerve pairs, 5 lumbar nerve pairs, and a single tailbone nerve pair (coccyx). Each pair exits through the vertebrae and innervates various parts of the body:
(1) The cervical spinal cord (C1 – C8) – nerves emerging from it innervate the back of the head, the neck and shoulders, the arms and hands, and the diaphragm.
(2) The thoracic spinal cord (T1 – T12) – nerves emerging from it innervate the chest muscles, some muscles of the back, and many organ systems, including parts of the abdomen.
(3) The lumbar spinal cord (L1 – L5) – nerves emerging from it innervate the lower parts of the abdomen and the back, the buttocks, some parts of the external genital organs, and parts of the leg.
(4) The sacral spine (S1 to S5) – nerves emerging from it innervate the thighs and lower parts of the legs, the feet, most of the external genital organs, and the area around the anus.
Each spinal cord segment controls different body functions; therefore, the injury is categorized according to its location. As much as the injury is closer to the neck, it will typically cause extensive disability and paralysis throughout a larger part of the body, including the limbs (tetraplegia/quadriplegia). A lower injury along the spinal cord can cause paralysis in the entire lower part of the body, including the legs (paraplegia).
In addition, a spinal cord injury can be complete or incomplete. The former involves the absence of any motor, sensory, or autonomic function below the level of the injury. An incomplete injury, on the other hand, means that the ability of the spinal cord to convey signals to or from the brain is not completely lost, and usually, patients retain some motor or sensory function below the injury.
Will I Be Able to Get an Erection Following a SCI?
A spinal cord injury can lead to sensory changes and likewise affect sexual desire, the ability to get and maintain an erection, achieve orgasms, and ejaculate. This is why, for many men, the first question that comes into mind after a SCI is: will I be able to get an erection and continue to have sexual intercourse?
As for achieving and maintaining erections, the spinal cord has two areas that impact this ability: the T11-L2 and the S2-S4 segments. In the case of a SCI, its impact on sexual function will depend on its exact location, the extent of damage to the nerve fibers, and whether the injury is complete or incomplete. With incomplete injuries, individual cases must be considered since there are many possible variations among patients regarding the degree of sexual function.
There are two types of erections, and a SCI can impact either one or both:
- Psychogenic erections – the brain is the source of psychogenic erections, which are triggered by sights, sounds, thoughts, and even smells (such as perfumes) that are sexually arousing (mental stimulation). The area in the spinal cord responsible for psychogenic erections is located at segment T11-L2 (see Illustration 1). As long as it is not injured, a man may get an erection from mental stimulation whereby a neural impulse goes through the spinal cord to the peripheral nerves and from there to the penis – where a chain of reactions triggers an increase in blood flow to the organ, followed by an erection. However, when this sexual center is injured (an injury above L2), the neural impulse from the brain cannot pass to the penis through the damaged part of the spinal cord, and as long as the injury is complete, a psychogenic erection cannot be achieved. However, it’s important to remember that in most cases of injuries below L2, a man may still get reflexogenic erections. Additionally, for men that can still get psychogenic erections, although they may be long-lasting and the penis often gets longer and fuller, it might not be rigid enough for full sexual intercourse.
What can be done to encourage a psychogenic erection? Focus on enhancing mental stimulation. You can ask your partner to help you get aroused with sights, sounds, and smells that arouse you.
- Reflexogenic (reflex/spontaneous) erections– come from direct stimulation of the penis or other erotogenic organs (such as the nipples, ears, etc.’) and can occur without erotic thoughts. The ability to achieve a reflexogenic erection is controlled by the sexual center located in segments S2-S4 in the lower back (see Illustration 1). If this segment remains intact, neural impulses from penile stimulation can pass through it and cause an erection. Likewise, when the injury is above S2, a man may still be able to get a reflexogenic erection, provided the nerve fibers below S2 (S2 through S5, for example) are still intact. Often reflexogenic erections are large and rigid enough for full sexual intercourse, though they may not last long, and repeated penile stimulation might be needed. Some men with SCI may notice a reflexogenic erection when penile stimulation is not sexual, such as when changing a catheter, cleaning their genitals, or even when getting dressed or pulling a blanket over their body.
What can be done to encourage a psychogenic erection? Focus on physical stimulation. Try using of vibrators, various sex toys, and constrictive penis rings to increase penile blood flow.
Illustration from the hollister.com
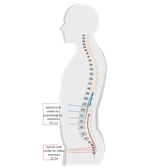
Illustration 1 – the erectile control centers in the spinal cord
In conclusion, it appears that many men with a SCI can achieve a particular type of erection. The extent of the injury and its location on the spinal cord will determine the type of erection (one triggered by mental stimulation or one achieved by direct penile stimulation). In addition, your physician may suggest various treatment options similar to those applicable in cases of erectile dysfunction, such as PDE5 medications, penile pumps, penile injections, and penile implant surgery.
The Company hereby clarifies that the information contained on the website is for informational purposes only, and is not intended to be a substitute for professional medical and healthcare advice, and does not constitute medical advice or opinion. Always seek the advice of your physician or other qualified health provider with any medical condition or question you may have regarding a medical condition.


