

14.04.2022 - Vertica® experts
Cipralex and sexual dysfunction
Why do antidepressant medications such as Cipralex (Escitalopram) cause sexual
Impotence, or Erectile Dysfunction is a chronic (ongoing) problem with a man’s sexual functioning, characterized by the inability to obtain or maintain an erection rigid enough for satisfactory sexual intercourse. Impotence can vary with respect to its severity, ranging from a mild disorder to the complete absence of an erection. This is a very common medical condition, especially in older men, and it is estimated that 350 million men worldwide are affected by impotence to some degree or another. In the past, it was believed that impotence is mainly caused by psychological problems. However, today it is known that among most men impotence is caused by physical problems. It is very important to treat it because it is a condition that may be a symptom (sometimes the first) of accompanying diseases in other systems of the body, or alternatively a predictive factor for cardiovascular disease in the future. Apart from this, impotence can have a significant effect on a man’s sexual and general health, as well as that of his partner, with respect to both the physical and psychological aspects.
Data about impotence | How is an erection generated? | Self-diagnosis of impotence | Reasons for impotence | Symptoms of impotence | Medical diagnosis of impotence | Treatment for impotence | Explanation in the video about impotence | Common questions about impotence
↵
↵
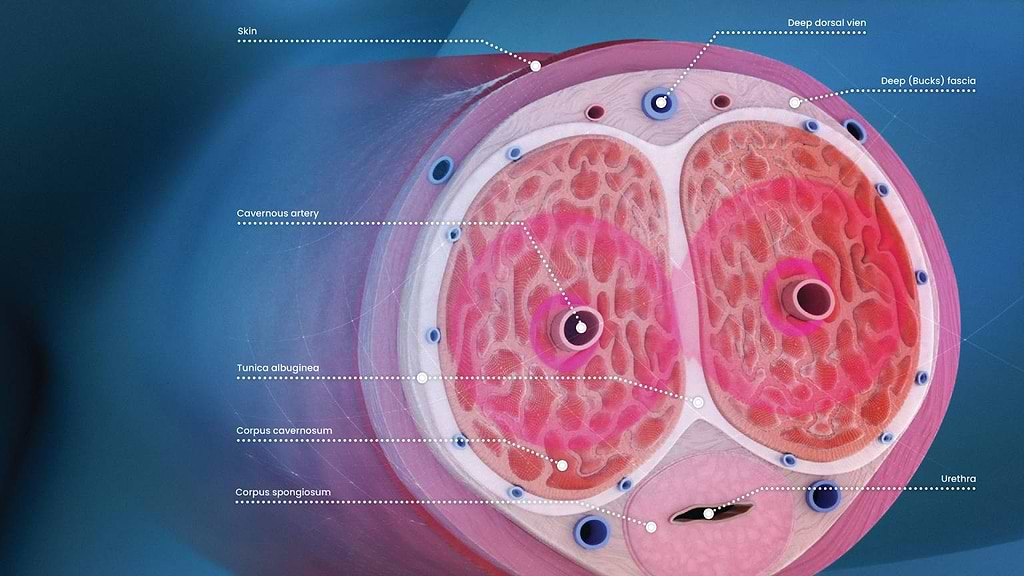
The penis comprises two cylindrical bodies called the corpora cavernosa that are essentially the erectile bodies. These bodies are composed of cavities of many blood vessels (creating a tunnel-like appearance), and whose walls are made of muscle tissue. An erection occurs when:
Damage to each of these mechanisms (the anatomical, nervous, hormonal or the one related to the role of the blood vessels) can damage the mechanisms responsible for creating and maintaining a stiff erection, which manifests as impotence.
↵
Although impotence is a very common problem, it is important to understand that it is only one component of a whole complex of male sexual dysfunction disorders, and sometimes it is easy to confuse it with other problems in sexual function that may occur in parallel, such as: decreased libido, problems related to ejaculation (such as premature ejaculation and delayed ejaculation), anorgasmia (inability to reach orgasm) and more.
The clearest symptom of impotence is an erection problem, or, in other words, the inability to achieve a stiff erection or the inability to maintain a stiff erection throughout sexual activity. (See below for details about the symptoms of impotence.) However, it is important to understand that there is a difference between one occasion to a few isolated occasions of no erection (such as on a background of drinking alcohol, drug consumption, great stress, problems in a relationship or simply because of fatigue or when distracted), and the development of a continuous pattern of chronic erectile dysfunction.
If you suspect that you suffer from impotence, it is always important to consult with the physician treating you in order to reach the correct diagnosis and obtain the most appropriate treatment. A full medical diagnostic evaluation is also important if there are accompanying health problems such as cardiovascular disease, diabetes, high blood pressure, and more, since in many cases impotence is a symptom of these problems, occasionally long before they are known about.
↵
Impotence problems can occur due to a range of different health conditions which are important to diagnose and treat. It is acceptable to divide the causal factors in to physical ones (organic), psychological/mental (psychogenic) ones, or a combination of both.
Around 8 out of 10 cases of impotence have an organic cause, most due to conditions which cause a decrease in blood flow to the penis:
Anatomical problems in the penis such as:
Mental/emotional problems are the cause in about 1 in 10 cases of chronic impotence.
For the most part, psychogenic impotence comprises symptoms that appear suddenly, and the condition could be resolved when the mental problem itself is treated (for example, depression or anxiety). There are men whose response to impotence is increased depression or anxiety; this is likely to create a vicious circle: impotence –> a worsening mental state –> chronic impotence.
Also, in case where they occasionally manage to achieve a hard erection (such as spontaneous erections during the night, a morning erection or an erection through masturbation), it is reasonable to suppose that the cause for impotence is psychological.
↵
In most cases, impotence is a problem that develops over time, and usually, the man will experience occasional problems with his erection, with a gradual worsening of erectile function. The symptoms of impotence include:
A persistent inability to achieve an erection sufficiently hard for pleasurable sexual activity is an obvious symptom of impotence. However, contrary to popular belief, impotence is not exactly a condition in which an erection cannot be achieved at all. It is also defined as impotence in situations where achieving an erection is sometimes possible, but not on every occasion when wishing to have sex.
This is a situation in which the man manages to achieve a stiff erection, but it is not maintained for long enough (to achieve penetration or to have satisfying intercourse). Symptoms of impotence are both in cases where the erection “falls” immediately and whether it “comes and goes” intermittently.
One of the signs that the cause of impotence is psychological is a state of being unable to reach orgasm before the erection is lost. It is possible that the problem is general anxiety, performance anxiety, stress or fear of failure in bed. These are also symptoms of impotence.
As mentioned, impotence can vary with respect to its severity, ranging from a mild disorder to the complete absence of an erection; therefore, even partial erections are a symptom of impotence. One of the recognized ways of assessing erection hardness is through the EHS index (Erection Hardness Score) – a simply applied tool for grading erection hardness on a scale of 0-4:
Score 0 – The penis does not expand and grow
Score 1 – The penis grows but does not become hard at all
Score 2 – The penis becomes hard, but not enough for penetration
Score 3 – The penis is hard enough for penetration, but not fully hard
Score 4 – The penis is fully hard
↵
In the process of the initial diagnosis of impotence, the doctor will perform an in-depth questioning regarding the patient’s general health, including in the context of underlying diseases, identifying signs of hormonal problems, and more. Thereafter, a physical examination will be performed, during which the doctor will assess if there are signs indicating disruption of blood flow to the penis. An examination of the penis will be carried out, as well as a rectal examination.
If there is a suspicion of a specific origin of the problem, the physician will investigate it in more depth. For example, if there is a suspected neurological problem (nervous), the patient will be referred for more in-depth neurological tests; if disruption to normal blood flow to the penis is suspected, it is possible that the patient will be referred for a Doppler ultrasound examination. Should there be a suspected hormonal imbalance, it is possible that the patient will be referred for an in-depth investigation by an endocrinologist.
Read more about the Impotence Test »
↵
These medicines are the first line of treatment for erectile disorders. They belong to the “PDE5 enzyme inhibitor” drug family, whose use is very common. The mechanism of action: increasing blood flow to the penis by affecting the cGMP molecule involved in the relaxation and dilation of the arterial blood vessels in the penis during sexual stimulation, thereby improving blood flow to the penis and creating a stiff erection (see explanation above). The drugs are mainly effective in cases where there is partial damage to the arterial blood vessels bringing blood to the penis, and they are taken around an hour or two prior to having sex.
This is a cylinder-like device that is used before intercourse. The mechanism of action of the device: when the penis is inserted into the cylinder and the device is activated, there is a pump that sucks out and removes the air from it until a vacuum (empty space) is created. The Vacuum results in elevated blood flow to the penis, thus creating an erection. After removing the device, in order to keep the blood in the erectile bodies, an elastic rubber ring is worn on the base of the penis. The erection is maintained for around 30 minutes, after which, the elastic ring should be removed from the penis.
The treatment is based on the injection of a drug into the sides of the body of the penis, and is performed by the patient himself. Mechanism of action: the drug contains substances which cause the relaxation of the smooth muscles in the erectile bodies (corpora cavernosa), to dilate the arterial blood vessels and thereby increase blood flow to the penis and create an erection. Injection Treatment was common, especially at the time when no drug treatment for impotence existed.
These are tiny suppositories that are inserted into the urethral opening of the penis. Mechanism of action: the drug contains substances which cause the relaxation of the smooth muscles in the erectile bodies, to dilate the arterial blood vessels and thereby increase blood flow to the penis and create an erection – usually within 10-15 minutes. However, the efficacy of the suppositories is less than that of the injections.
This involves low-energy acoustic waves. Over the years, shock waves have been used for various medical situations, but only in recent years, in Israel, has use of this technology for impotence been developed. The potential mechanism of action: The shock waves transferred to the erectile bodies encourage the formation of new blood vessels through which blood flow to the penis improves. The treatment is performed using a special device for passing shock waves to a number of regions in the body of the penis. The treatment extends over 12 stages and is carried out in private clinics or hospitals.
Treatment with radio waves has existed for years, whether for the purpose of cauterizing tissues with high energy or as a dermatological treatment to improve the appearance of loose skin and wrinkles using low energy radio waves. Vertica®, a medical device for the home treatment of impotence was launched for the first time in 2021. The device is based on the use of low intensity radio waves to rehabilitate the tissue in the penis (the tunica albuginea) which constitutes part of the physiological mechanism of an erection. The tunica albuginea contains collagen protein fibers that give it strength and flexibility. However, with age, the collagen fibers in the tunica albuginea become worn out and weaken. As a result, the tunica cannot effectively block the blood being drained through veins in the erectile bodies during sexual arousal, and as a result, blood leaks out of the penis, and the erection either becomes significantly weaker or it is lost. The mechanism of action of the device: radio waves essentially release low frequency energy (1 megaHertz). When the energy is released, it creates heat that warms the deep tissues. Heating the tunica albuginea tissue in the penis encourages the production of collagen protein whose function is to give the tissue stiffness and firmness, and thereby contributing to the restoration of the physiological erection mechanism.
The implant is constructed from two cylindrical bodies that are implanted into the corpora cavernosa of the penis, and in effect, replace the natural erection mechanism. There are two types of implant:
On the one hand, they provide the penis with constant rigidity, but on the other hand, they are flexible enough to bend it during the day and then straighten it before having sex.
Constructed from two cylindrical bodies implanted inside the corpora cavernosa of the penis, a pump implanted in the scrotum, and a container implanted in the pelvis which contains fluid. When an erection is desired, pump located in the scrotum is pressed, transferring fluid from the implanted container to the cylindrical bodies that are fill with fluid; they stretch and thicken in the process, and a stiff erection is obtained. Pressing a button on the pump releases the fluid from the cylindrical bodies back into the container, and the penis goes flaccid. An implant of this kind allows for a more natural erection. To read about penile implant surgery in depth
This surgery is intended for situations of impotence caused a blockage in one main artery carrying blood to the penis, and is only performed when the patient has no other background risk factors. The surgery assists in improving blood flow to the penis by bypassing the area of the blocked artery.
Plasma is the liquid component of the blood which comprises half of its volume. It contains different components of the blood found in a dissolved state; it is rich in platelets that have an important role in clotting of the blood, and also contain blood proteins, among them “growth factors” that assist in the processes of tissue healing following an injury, electrolytes (such as calcium, magnesium and sodium), hormones, oxygen, and more. The mechanism of action of PRP treatment: the treatment is designed to help in situations of impotence by enriching the tissues in the penis with plasma components to make them “healthier” such that they perform their function properly. In order to prepare PRP, a small sample of blood is required from the patient. The blood sample is placed in a centrifuge in order to separate the plasma and the platelets from the other components of the blood. In this way, plasma with a particularly high concentration of platelets (PRP) is obtained, which is injected into the patient’s penis (P-shot).
Stem cells are unique cells that can differentiate into endothelial cells (which line the inner layer of the blood vessels), nerve cells, or smooth muscle cells. The potential mechanism of action of stem cells in cases of impotence: restoration of the natural erectile mechanisms by the growth of healthy tissue generated by the stem cells. So far, the efficacy and safety of stem cell therapy has been proven in some studies of animals and humans with erectile dysfunction. However, more studies are needed to understand the full potential for the treatment of impotence. As of June 2022, there are medical centers that have started experimental treatments for impotence problems by injecting stem cells into the corpora cavernosa of the penis.
These are treatments for impotence with a psychogenic cause, as a result of great stress, anxiety disorder, performance anxiety, depression or problems in the marital relationship that impact emotionally. The treatment methods include psychological treatment, psychotherapy, and professional sexual counselling (either individually or with a partner) from a sexologist.
↩ [1] Chitaley K, Kupelian V, Subak L, Wessells H. Diabetes, obesity and erectile dysfunction: field overview and research priorities. J Urol. 2009 Dec;182(6 Suppl):S45-50. doi: 10.1016/j.juro.2009.07.089. PMID: 19846136; PMCID: PMC2864637.
↩ [2] Rastrelli G, Maggi M. Erectile dysfunction in fit and healthy young men: psychological or pathological? Transl Androl Urol. 2017 Feb;6(1):79-90. doi: 10.21037/tau.2016.09.06. PMID: 28217453; PMCID: PMC5313296.
The Company hereby clarifies that the information contained on the website is for informational purposes only, and is not intended to be a substitute for professional medical and healthcare advice, and does not constitute medical advice or opinion. Always seek the advice of your physician or other qualified health provider with any medical condition or question you may have regarding a medical condition.
With this self-test you can easily detect indications of erectile dysfunction. This test is based on the so-called IIEF-score. IIEF stands for «International Index of Erectile Function». In medicine, the IIEF-score is used to both diagnose erectile dysfunction and to monitor the effectiveness of therapeutic interventions. Take 2-3 minutes to complete the short questionnaire (6 multiple-choice questions) and see if you suffer from erectile dysfunction. There is no need to fill in personal details or identify yourself – we have no intention of using personal information.
14.04.2022 - Vertica® experts
Why do antidepressant medications such as Cipralex (Escitalopram) cause sexual

20.12.2021 - Ori Gidor
Morning Erection or “Morning Wood” (formally known as Nocturnal Penile
26.06.2022 - Vertica® experts
In the process of aging, many will develop a condition